Immunohistochemistry (IHC) remains a core method in hematopathology because diagnostically meaningful phenotypes can be resolved directly in tissue architecture, using antibody-defined lineage, differentiation, and proliferation markers. For any CE-IVD antibody or IHC antibody intended for clinical research/diagnostic workflows, evidence-based practice emphasizes analytic validation and control of pre-analytical and analytical variables to ensure accurate, reproducible readouts.
What CE-IVD antibodies for IHC in hematopathology are used to interrogate
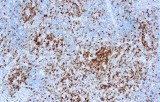
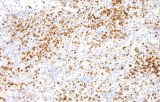
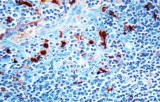
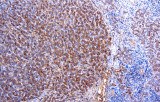
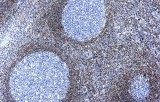
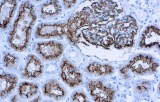
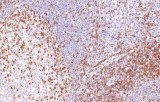
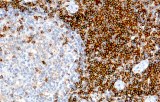
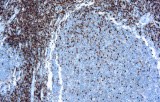
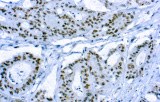
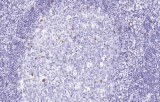
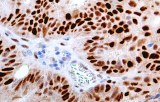
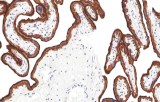
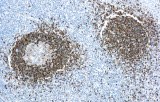
- Lineage assignment & major differentials: B-cell vs T-cell phenotyping (e.g., CD20 vs CD3), supported by nuclear B-cell transcription factors such as PAX5 when pan-B markers are weak/absent.
- Entity-oriented panels for lymphoid neoplasms:
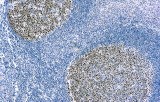
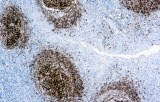
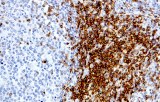
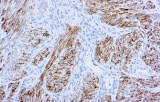
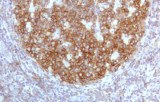
- Follicular lymphoma: typical co-expression patterns (e.g., CD10 with aberrant BCL2).
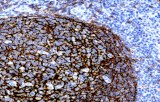
- CLL/SLL: characteristic co-expression of CD5 and CD23 in CD20+ B-cells (interpretation requires pattern awareness because reactive T-cells are present).
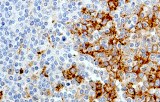
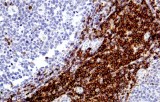
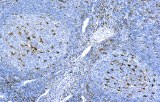
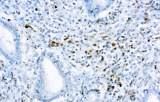
- Mantle cell lymphoma: cyclin D1 and SOX11 as key markers, including support for cyclin D1–negative cases.
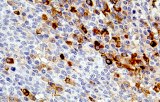
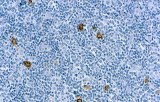
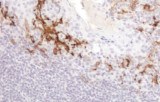
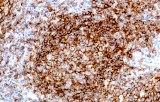
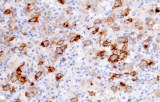
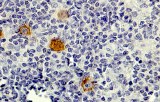
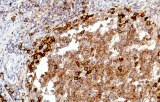
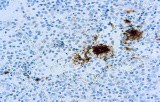
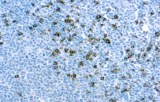
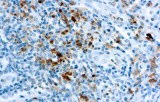
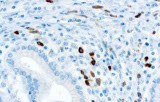
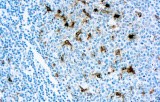
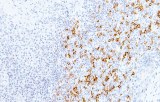
- Classic Hodgkin lymphoma: tumor cells typically CD30+ and often CD15+, with PAX5 weak and CD20 negative in large tumor cells.