Immunohistochemistry (IHC) is a well-established adjunct to histomorphologic evaluation for thyroid and parathyroid lesions. Its use is particularly relevant in small biopsies, metastatic work-ups, and cases with overlapping or limited architectural features. Thyroid and parathyroid neoplasms represent a substantial proportion of endocrine tumors encountered in routine surgical pathology practice within this anatomic region.
The application of CE-marked, in vitro diagnostic (IVD)–validated primary antibodies provides a regulated framework for the detection of lineage-associated and differentiation-related proteins in formalin-fixed, paraffin-embedded (FFPE) tissue. When implemented within laboratory-validated workflows and interpreted in conjunction with appropriate controls, these reagents support standardized analytical performance and clinically meaningful interpretation. As with all IVD reagents, laboratory-specific verification and contextual interpretation remain essential.
Key Immunohistochemical Markers in Thyroid and Parathyroid Pathology
Thyroid Lineage and Differentiation
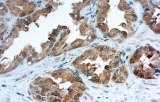
Thyroglobulin (Tg)
Thyroglobulin is widely used as a marker of differentiated thyroid follicular epithelium and is helpful in supporting thyroid origin in both primary and metastatic lesions. Expression may be reduced, focal, or absent in poorly differentiated or dedifferentiated thyroid carcinomas, and interpretation should take into account potential technical and contextual limitations.
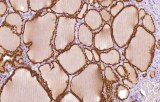
PAX8
PAX8 is a nuclear transcription factor expressed in thyroid follicular cells and is useful for supporting thyroid lineage, particularly in tumors with diminished or absent thyroglobulin expression. Interpretation requires awareness that PAX8 expression is not specific to thyroid tissue and may be observed in select non-thyroid epithelial neoplasms.
Medullary Thyroid Carcinoma
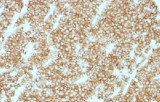
Calcitonin
Calcitonin is a principal immunohistochemical marker of parafollicular C-cell differentiation and is central to the diagnosis of medullary thyroid carcinoma in most cases. While it demonstrates high diagnostic utility in typical primary and metastatic settings, rare calcitonin-negative tumors have been reported, and results should be interpreted in conjunction with morphology, clinical findings, and additional ancillary studies when indicated.
Follicular-Derived Thyroid Lesions: Benign and Malignant
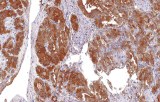
Galectin-3
Galectin-3 is among the most extensively studied immunohistochemical markers in thyroid pathology and is more frequently expressed in malignant follicular-derived tumors than in benign nodules. However, expression may also be observed in certain benign or inflammatory thyroid conditions. Accordingly, its diagnostic value is greatest when used as part of a multiparametric immunohistochemical panel rather than as a standalone marker.
Parathyroid Differentiation
Parathyroid Hormone (PTH)
Parathyroid hormone is a key marker for confirming parathyroid origin and is particularly useful in the differential diagnosis between parathyroid and thyroid lesions with overlapping histologic features. It supports lineage confirmation in parathyroid adenomas, carcinomas, and ectopic or intrathyroidal parathyroid tissue, with interpretation informed by morphologic and clinical correlation.
Considerations for CE-Marked / IVD-Validated Primary Antibodies
- Intended for clinical diagnostic use under the EU In Vitro Diagnostic Regulation (IVDR 2017/746).
- Support standardized analytical performance for lineage confirmation and tumor classification in thyroid and parathyroid pathology.
- Facilitate panel-based diagnostic approaches consistent with published pathology literature and practice recommendations.
- Require laboratory-specific verification, appropriate controls, and interpretation within the full clinicopathologic context, regardless of regulatory status.