Parathyroid hormone (PTH) is an 84–amino acid peptide hormone synthesized as prepro-PTH and produced predominantly by parathyroid chief cells. It is a central endocrine regulator of extracellular calcium and phosphate homeostasis. Physiologically, PTH secretion is tightly regulated by circulating ionized calcium via calcium-sensing receptor–mediated mechanisms in the parathyroid gland, enabling rapid defense against hypocalcemia. In target organs, PTH exerts well-established actions on the kidney (renal tubular calcium handling and phosphate excretion) and the skeleton (coupling bone remodeling to mineral homeostasis). In diagnostic pathology, PTH expression serves as a useful indicator of parathyroid differentiation, while recognizing that staining intensity and distribution may vary across lesions.
Diagnostic utility of PTH immunohistochemistry in thyroid and parathyroid pathology
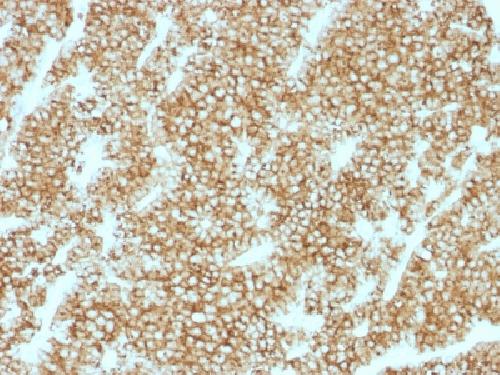
In surgical pathology, parathyroid hormone immunohistochemistry (PTH IHC) is widely used as an adjunct to morphology to support parathyroid lineage assignment when anatomic location and histologic features create diagnostic ambiguity—particularly in cases of intrathyroidal or ectopic parathyroid tissue and neck masses closely associated with the thyroid gland. A practical example is incidental intrathyroidal parathyroid tissue, in which PTH IHC highlights parathyroid chief cells and supports correct classification.
PTH immunostaining is also applied in cytology and other limited-material workflows to aid in the distinction between parathyroid and thyroid lesions, which may overlap cytomorphologically. Studies evaluating thyroid versus parathyroid lesions have shown that PTH immunostains and related PTH-based approaches can be valuable adjuncts in resolving diagnostically challenging cases.
Importantly, PTH expression in parathyroid tumors may be heterogeneous, and staining intensity can vary within and between lesions. Although PTH immunoreactivity is demonstrable in the majority of parathyroid neoplasms in routine FFPE immunohistochemistry, rare nonfunctional parathyroid carcinomas may show absent or only focal PTH staining. Accordingly, a negative PTH IHC result does not categorically exclude parathyroid origin and should be interpreted in conjunction with morphologic findings and additional immunohistochemical markers.
Key features to consider in anti-PTH antibodies for IHC applications
For anti-PTH antibodies used in clinical immunohistochemistry for thyroid and parathyroid pathology, published IHC validation frameworks and pathology practice guidelines emphasize performance characteristics that directly affect diagnostic reliability:
-
Appropriate biological signal: staining patterns consistent with expected PTH expression in parathyroid chief cells, supporting lineage assessment in ectopic or intrathyroidal settings.
-
Analytical validation in FFPE IHC: use of appropriate positive and negative controls, confirmation of expected cellular localization, and method-level validation to ensure reproducible staining performance.
-
Utility in differential diagnosis: ability to contribute meaningfully to thyroid–parathyroid discrimination when used as part of an integrated immunohistochemical panel.
-
Transparent disclosure of limitations: documentation of potential staining heterogeneity and recognition that rare PTH-negative parathyroid carcinomas can occur, informing cautious interpretation and reflex testing strategies.