Carcinoembryonic antigen (CEA), also known as CD66e, is a glycoprotein widely used as a tumor marker in immunohistochemistry (IHC). It plays roles in cell adhesion, differentiation, anoikis, polarization, and maintenance of tissue architecture. CEA is normally expressed in fetal tissues such as fetal colon and is highly upregulated in many adenocarcinomas of the gastrointestinal tract, lung, and breast. In gynecological tissues, CEA may be expressed in a subset of ovarian and endocervical adenocarcinomas.
Diagnostic Value of Anti-CEA Antibodies in Gynecological Pathology
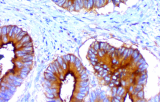
In gynecological pathology, Anti-CEA antibodies are used as part of IHC panels to support the diagnosis and differentiation of adenocarcinomas. CEA staining can help distinguish endocervical adenocarcinomas and some ovarian adenocarcinomas from other malignancies such as endometrial adenocarcinomas or mesothelioma. Combined with markers such as Calretinin, CK5/6, D2-40, HBME-1, Napsin A, MOC-31, and Ber-EP4, CEA contributes to a reliable diagnostic panel for differentiating adenocarcinoma from morphologically similar entities and for identifying the primary site in metastatic tumors.
Key Features and Clinical Implications
- CEA is a supportive marker for adenocarcinomas in the gastrointestinal tract and in certain gynecological tumors.
- It aids in differentiating adenocarcinomas (CEA-positive) from mesothelioma (CEA-negative).
- Anti-CEA immunostaining is valuable as part of a panel to identify the origin of metastatic adenocarcinomas.
- While CEA expression may correlate with tumor progression in some cancers, its routine use for monitoring gynecological cancers is limited; other markers such as CA-125 are more commonly used.
- Integrating Anti-CEA with other IHC markers enhances diagnostic accuracy in challenging gynecological cases.
