The Wilms Tumor 1 (WT1) protein is a zinc-finger transcription factor originally characterized as a tumor suppressor gene critical for kidney and genitourinary development. In diagnostic pathology, Anti-WT1 CE/IVD antibodies for Immunohistochemistry (IHC) are essential reagents for detecting WT1 expression in formalin-fixed, paraffin-embedded tissue sections. These IVD-marked (In Vitro Diagnostic) antibodies are widely used by clinical laboratories and research institutions to aid in tumor classification, differential diagnosis, and prognostication across a variety of neoplastic and non-neoplastic conditions.
WT1 immunostaining has evolved into a standard biomarker assay due to its robust performance in identifying nuclear protein expression in tumor cells, making it indispensable in pathology workflows where specific, sensitive IHC assays are required for accurate diagnosis.
Biological and Pathological Significance of WT1
WT1 is expressed in normal mesothelial cells, renal podocytes, hematopoietic progenitors, and reproductive tract stromal cells, reflecting its role in tissue development and differentiation. In the context of human neoplasia:
- WT1 is highly expressed in Wilms tumor, a pediatric renal cancer, providing a historically significant diagnostic target.
- WT1 expression is a reliable marker for malignant mesothelioma, especially in epithelioid subtypes, where nuclear WT1 positivity distinguishes mesothelioma from metastatic adenocarcinomas.
- WT1 immunoreactivity has been reported in ovarian serous carcinomas, soft tissue sarcomas, and select solid tumors, expanding its utility in diagnostic pathology beyond embryonal tumors.
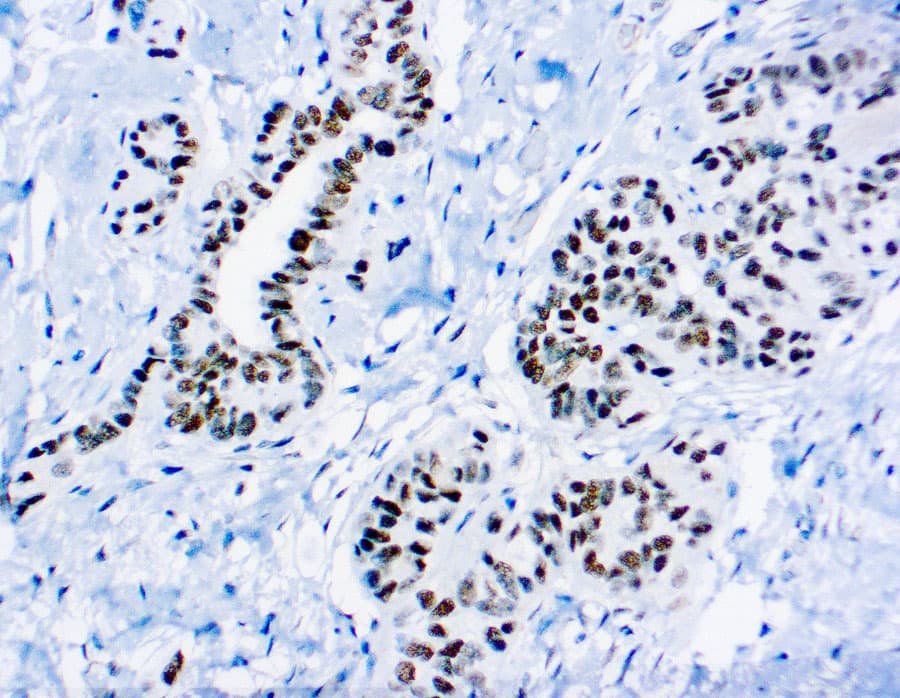
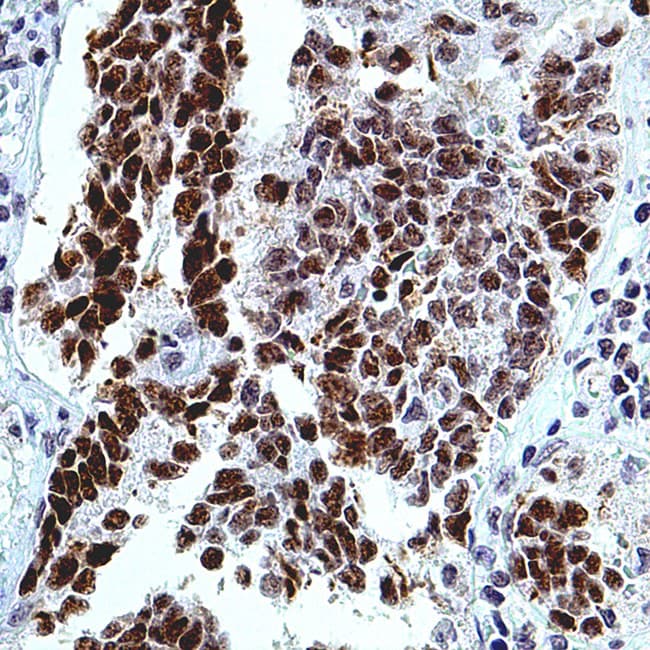
The subcellular localization of WT1 is clinically relevant: nuclear staining is considered diagnostically meaningful, whereas cytoplasmic staining may represent non-specific background or physiologic expression in certain cell types.
Key Features of Anti-WT1 CE/IVD Antibodies for IHC
Anti-WT1 CE/IVD antibodies are primary monoclonal or polyclonal immunoglobulins validated for clinical IHC use. Their critical features include:
- CE/IVD certification, ensuring compliance with regulatory standards for clinical diagnostics in the EU.
- High specificity for WT1 antigen, targeting multiple epitopes of the full-length protein or selected domains to capture all clinically relevant isoforms.
- Optimal performance on formalin-fixed, paraffin-embedded (FFPE) tissues, the standard preparation in histopathology laboratories.
- Compatibility with automated IHC platforms and manual staining workflows, facilitating integration into routine diagnostic protocols.
Diagnostic Applications and Utility
Mesothelioma and Differential Diagnosis
- Malignant pleural mesothelioma: WT1 nuclear positivity supports diagnosis, especially in epithelioid variants, with high specificity when included in an IHC panel.
- Distinguishes mesothelioma from adenocarcinomas of lung and other origins, where WT1 nuclear staining is rarely present.
Pediatric Tumor Evaluation
- In Wilms tumor (nephroblastoma), WT1 immunostaining aids in identification and subtyping of blastemal components.
Soft Tissue and Gynecologic Pathology
- WT1 expression has been observed in soft tissue sarcomas and is being explored as a prognostic marker.
- In gynecologic pathology, WT1 helps differentiate serous carcinoma from other histotypes and can provide prognostic insights in endometrial and ovarian tumors.
Panel Marker Integration
WT1 is commonly included in multiplex IHC panels, alongside calretinin, cytokeratin 5/6, and other lineage markers, to improve diagnostic accuracy in complex cases of pleural, peritoneal, and gynecologic tumors.