Hairy cell leukemia (HCL) is a rare, indolent mature B-cell neoplasm defined by distinctive morphology, immunophenotype, and the presence of the BRAF V600E mutation in the vast majority of classical cases. In hematopathology, immunohistochemistry (IHC) is essential for accurate diagnosis and for differentiating HCL from other splenic B-cell lymphomas.
Biological Significance of HCL
- Clonal proliferation of mature B lymphocytes with characteristic “hairy” cytoplasmic projections.
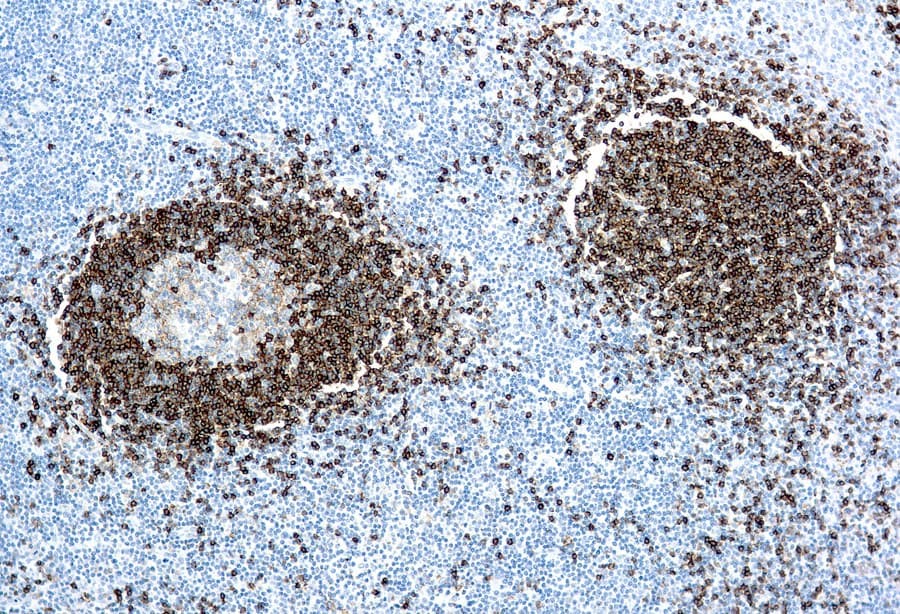
- Typical immunophenotype: CD20, CD22, CD11c, CD25, CD103, with frequent CD123 expression.
- BRAF V600E mutation acts as a key molecular driver in classical HCL.
- Annexin A1 is highly specific and supports distinction from related entities.
Diagnostic Utility of HCL IHC
- IHC in hematopathology complements morphology and flow cytometry, especially in bone marrow biopsies with fibrosis or low tumor burden.
- Anti-BRAF V600E and Annexin A1 antibodies provide strong diagnostic support, with performance dependent on assay conditions.
- Key IHC panels for HCL diagnosis:
- Positive: CD20, CD11c, CD25, CD103, CD123, Annexin A1
- Negative: CD5, CD10 (typically absent)
- Critical for differential diagnosis:
- Classical HCL vs. HCL variant (often BRAF-negative, CD25-negative)
- HCL vs. splenic marginal zone lymphoma
Key Features of Anti-HCL CE/IVD Antibodies
- Validated for FFPE tissues in hematopathology workflows.
- High-specificity clones for reliable detection.
- Effective in low tumor burden samples, depending on validation.
- CE/IVD compliance ensures reproducibility and regulatory alignment.
- Compatible with multiparametric IHC panels and integrated diagnostic workflows.